Fill in a Valid Care 1St Arizona Prior Authorization Template
The Care 1st Arizona Prior Authorization form is a critical document designed to streamline the process for individuals seeking healthcare coverage, specifically for those who are disabled, working, and aged between 16 and 65. This form covers a wide array of information necessary for the application, including personal details, employment and income data, and information about any other health insurance coverages. Applicants are required to provide detailed information about their health condition, the languages they are comfortable with for communication, and consent to interpreter services if needed. Additionally, the form inquires about the applicant's financial assets, any other sources of income, and whether they have applied for or received any disability benefits. The importance of accurate and truthful disclosure is emphasized, with a warning about potential fraud and the implications of providing false information. The commitment to nondiscrimination and the process for contesting decisions through a Fair Hearing are also outlined, ensuring applicants are aware of their rights and responsibilities throughout the process.
Care 1St Arizona Prior Authorization Preview
BHSF Form
Rev. 04/05
Prior Issue Obsolete
II
For Agency Use Only
Request date |
|
(Application date) |
Date mailed
Agency Rep
To protect your application date, we must receive this application by |
|
. |
(for agency use only)
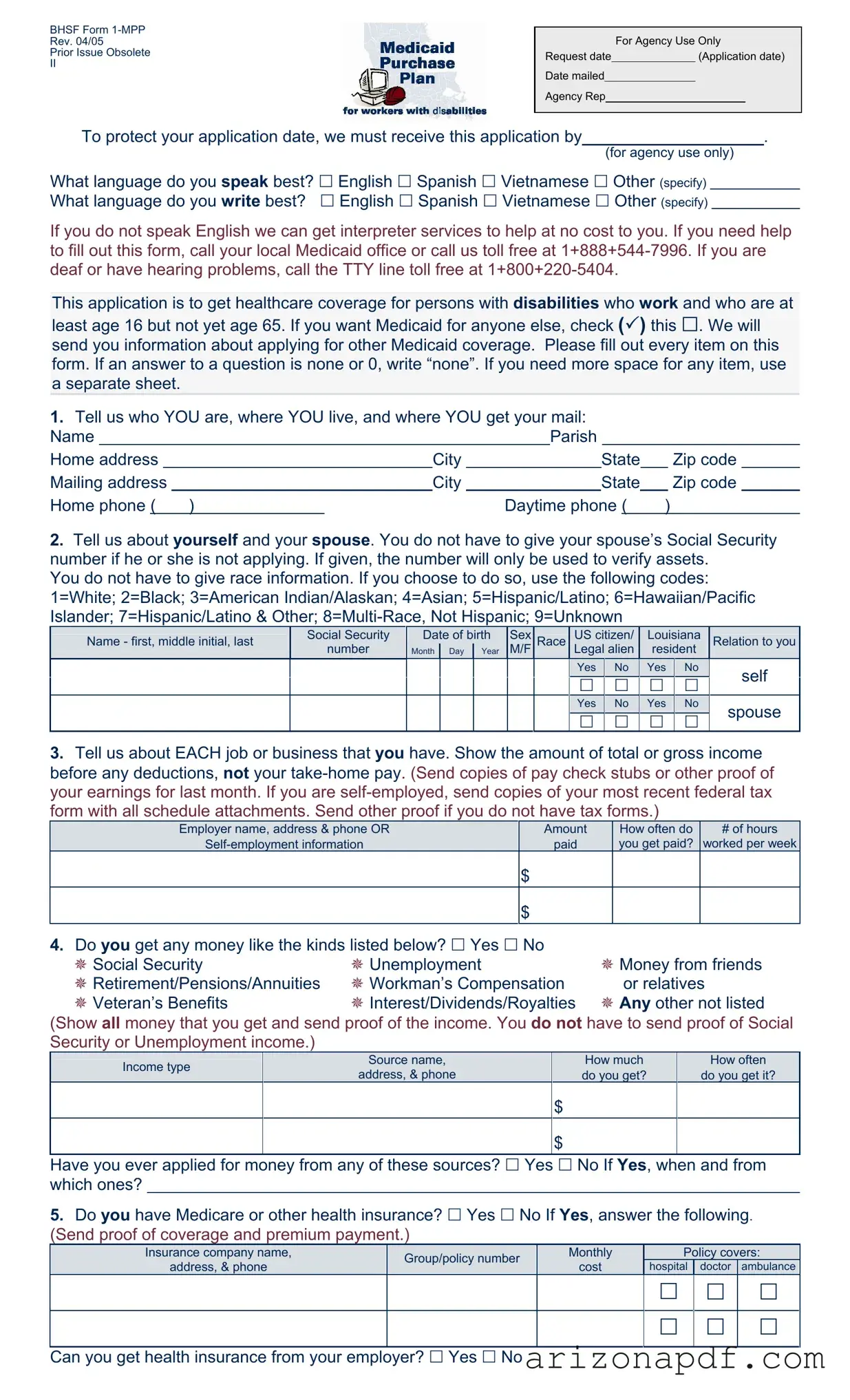
What language do you speak best? English Spanish Vietnamese Other (specify) What language do you write best? English Spanish Vietnamese Other (specify)
If you do not speak English we can get interpreter services to help at no cost to you. If you need help to fill out this form, call your local Medicaid office or call us toll free at
This application is to get healthcare coverage for persons with disabilities who work and who are at
least age 16 but not yet age 65. If you want Medicaid for anyone else, check ( ) this . We will send you information about applying for other Medicaid coverage. Please fill out every item on this form. If an answer to a question is none or 0, write “none”. If you need more space for any item, use a separate sheet.
1.Tell us who YOU are, where YOU live, and where YOU get your mail:
Name |
|
|
|
Parish |
|
|
|
|
||||||
Home address |
|
City |
|
|
State |
|
Zip code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing address |
|
City |
|
|
State |
|
Zip code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Home phone ( ) |
|
Daytime phone ( |
) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.Tell us about yourself and your spouse. You do not have to give your spouse’s Social Security number if he or she is not applying. If given, the number will only be used to verify assets.
You do not have to give race information. If you choose to do so, use the following codes: 1=White; 2=Black; 3=American Indian/Alaskan; 4=Asian; 5=Hispanic/Latino; 6=Hawaiian/Pacific Islander; 7=Hispanic/Latino & Other;
Name - first, middle initial, last |
Social Security |
Date of birth |
Sex |
Race |
US citizen/ |
Louisiana |
Relation to you |
||
|
number |
Month |
Day |
Year |
M/F |
|
Legal alien |
resident |
|
|
Yes |
|
No |
|
Yes |
|
No |
|
self |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|||||||
|
Yes |
|
No |
|
Yes |
|
No |
|
spouse |
|
|
|
|
|
|
||||
3.Tell us about EACH job or business that you have. Show the amount of total or gross income before any deductions, not your
Employer name, address & phone OR |
Amount |
How often do |
# of hours |
paid |
you get paid? |
worked per week |
$
$
4.Do you get any money like the kinds listed below? Yes No
Social Security |
Unemployment |
Money from friends |
Retirement/Pensions/Annuities |
Workman’s Compensation |
or relatives |
Veteran’s Benefits |
Interest/Dividends/Royalties |
Any other not listed |
(Show all money that you get and send proof of the income. You do not have to send proof of Social Security or Unemployment income.)
|
Income type |
|
Source name, |
|
|
How much |
|
How often |
|
|
|
address, & phone |
|
|
do you get? |
|
do you get it? |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
$ |
|
|
|
|
$
Have you ever applied for money from any of these sources? Yes No If Yes, when and from which ones?
5.Do you have Medicare or other health insurance? Yes No If Yes, answer the following. (Send proof of coverage and premium payment.)
Insurance company name, |
Group/policy number |
Monthly |
|
Policy covers: |
|||
address, & phone |
cost |
hospital |
doctor |
ambulance |
|||
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Can you get health insurance from your employer? Yes No
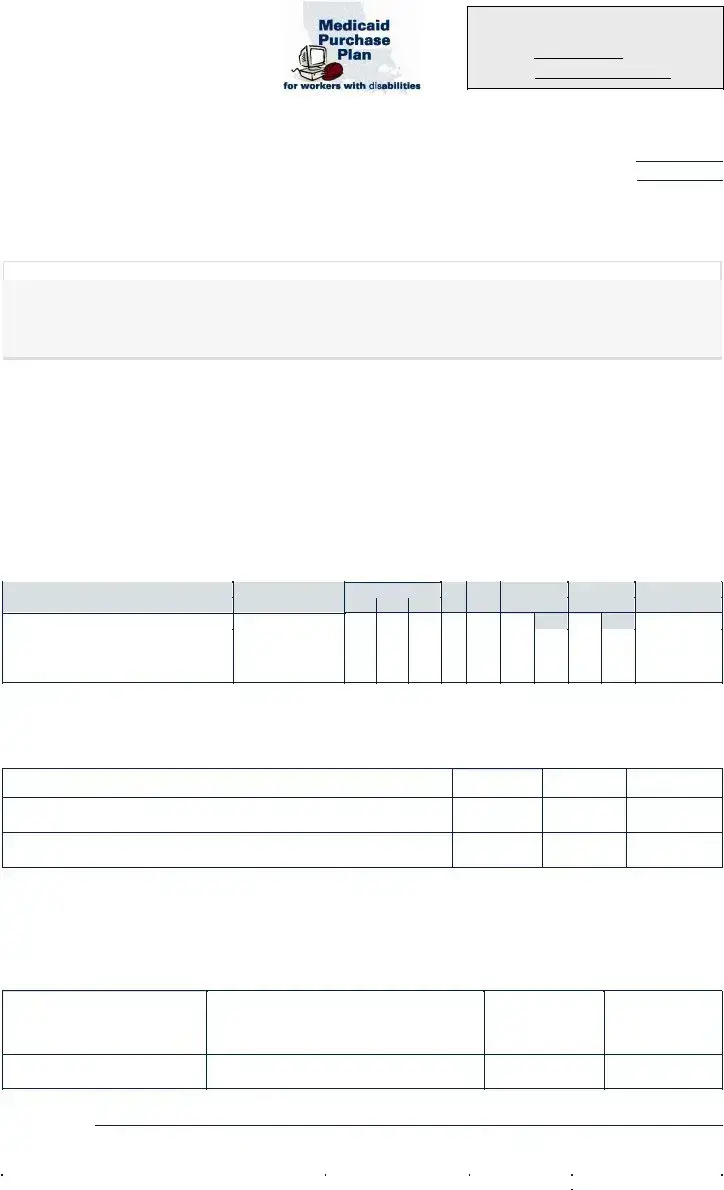
6.Do you, or you jointly with your spouse, have any assets or resources like those listed below? Yes No If Yes, give us the following information. (Send proof of ownership and value.)
|
Asset/Resource |
Company name, address, & phone; |
Value |
Amount owed |
|
||||
|
Account number and/or description |
|||
|
|
|
|
|
|
Checking/Savings accounts (type) |
|
$ |
|
|
|
|
|
|
|
Certificates of Deposit |
|
$ |
|
|
Retirement accounts |
|
$ |
|
|
Annuities/Trusts |
|
$ |
|
|
Stocks/Bonds |
|
$ |
|
|
Vehicles (if more than one) |
|
$ |
$ |
|
Property, other than your home |
|
$ |
$ |
|
Other (please be specific) |
|
$ |
$ |
7.Did you ever apply for or get Social Security Disability or Supplemental Security Income (SSI)
benefits? Yes No If Yes, when? |
|
Was a decision made? Yes No |
|
If Yes, what was the decision? |
|
|
|
|
|
|
|
8.What is your disability?
Tell us about the doctors or other medical providers who care for you:
Provider’s name(s)
Address & phone of this medical provider
9.Where did you find out about the Medicaid Purchase Plan?
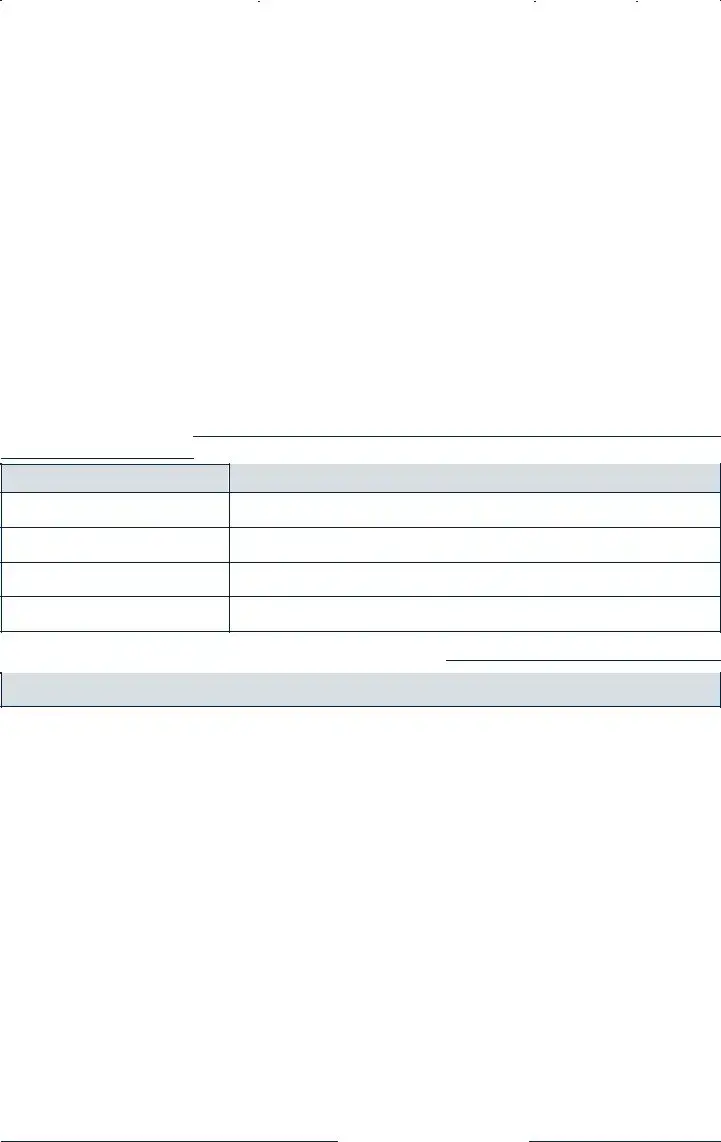
Rights and Responsibilities
I declare that I am a U.S. citizen or in this country legally.
The information I gave on this form is true and correct to the best of my knowledge. I realize if I knowingly give information that is not true OR if I knowingly hold back information, I may get health benefits for which I am not eligible. If that happens, I can be lawfully punished for fraud. I may also have to pay Medicaid back for any medical bills which are paid incorrectly.
I understand that the information I give about my situation will be checked. I agree to help do that, and to let Medicaid get information it needs from government agencies, employers, medical providers, and other sources. If I refuse to help with this process or in later reviews caused by reported changes, or as part of a Recipient Eligibility review, it will mean that I can’t get Medicaid until I do help.
I know that Social Security numbers will only be used to get information from other government agencies to prove my eligibility.
I agree to tell Medicaid within 10 days if 1) I move out of state; 2) there are changes in where I live or get my mail; 3) there are any changes in other health insurance coverage; 4) there is any change in my work status.
By accepting Medicaid, I agree that any medical payments received from other sources will be sent to the Department of Health and Hospitals for any services that were covered by Medicaid.
I can ask for a Fair Hearing if I think the decision made on my case is unfair, incorrect or being made too late.
Medicaid can’t treat me differently because of my race, color, sex, age, disability, religion, nationality or political belief. If I think they have, I can call the U.S. DHHS Regional Office for Civil Rights in Dallas, TX at
Signature of Applicant or Authorized Representative |
|
Date |
|
|
|
Signature of Agency Representative, if applicable |
|
Date |
File Properties
| Fact | Detail |
|---|---|
| Form Title | Care 1st Arizona Prior Authorization Form |
| Revision Date | April 2005 |
| Purpose | To get healthcare coverage for persons with disabilities who work, are at least 16 and not yet 65 years old. |
| Language Support | Supports multiple languages including English, Spanish, Vietnamese; interpreter services offered at no cost. |
| Contact Information | Local Medicaid office phone; Toll-free contact number; TTY line for deaf or hearing problems. |
| Eligibility Verification | Social Security numbers used only for eligibility verification from government agencies. |
| Rights and Responsibilities | Outlines applicant's responsibilities, fraud warning, agreement to report income, and rights to fair hearing, including nondiscrimination. |
| Governing Law(s) | Governed by laws pertaining to Medicaid and healthcare provision in the United States, specifically referencing the Department of Health and Hospitals for Louisiana. |
Instructions on Utilizing Care 1St Arizona Prior Authorization
Filling out the Care 1st Arizona Prior Authorization form is vital for individuals seeking healthcare coverage, especially for those with disabilities who work. This form serves as a comprehensive tool for evaluating one's eligibility for Medicaid under specific conditions, relating to age and working status. The process involves providing detailed personal information, employment and income details, current health insurance status, and other pertinent financial data. To ensure a smooth and accurate application process, follow these steps carefully.
- Start by indicating the language you are most proficient in speaking and writing at the top of the form. Choices include English, Spanish, Vietnamese, or Other. If 'Other,' specify the language.
- If you require interpreter services, remember that the agency can provide these at no extra cost. This information offers reassurance to non-English speakers about the accessibility of assistance.
- Fill in your contact information, including your name, home address, both city and state, zip code, and both your home and daytime phone numbers.
- Under the section about yourself and your spouse, provide names, Social Security numbers (optional for non-applying spouses but required for verifications), dates of birth, sex, and race. Note that providing race information is optional, and there are codes listed for race options.
- Disclose your US citizenship or legal alien status along with Louisiana residency status for both yourself and, if applicable, your spouse.
- For the employment section, list each job or business you and your spouse have, including the employer name, address, phone number, the amount of income before deductions, how often you are paid, and total hours worked per week. Attach copies of pay stubs or, for the self-employed, the most recent tax return.
- If you receive any form of additional income such as Social Security, unemployment benefits, etc., mark 'Yes' and provide the source, amount, and frequency of such income. Include proof except for Social Security or unemployment income.
- Detail any existing health insurance, including Medicare, under Section 5. Provide the insurance company's name, group/policy number, monthly cost, and what the policy covers. Attach proof of coverage and premium payments.
- In Section 6, disclose any assets or resources you own individually or jointly with your spouse, including checking/savings accounts, retirement accounts, vehicles, property (other than your home), and any other assets. Provide the company name, address, phone number, value, amount owed (if applicable), and the account number or description.
- If you have ever applied for or received Social Security Disability or Supplemental Security Income benefits, indicate this under Section 7, including the decision if one was made.
- Describe your disability in Section 8 and include information about your medical providers, such as names, addresses, and phone numbers.
- Under 'Rights and Responsibilities,' read and understand the declarations and agreements carefully. It's essential to acknowledge the accuracy of information provided and the consequences of fraud.
- Finally, sign and date the form at the bottom. If filled out with assistance from an agency representative, ensure their signature and date are also included.
Completing the Care 1st Arizona Prior Authorization form with attention to detail and accuracy is crucial for a successful application. Ensure all information is up-to-date and supported by the necessary documents. This thorough approach will facilitate a smoother review process and help secure the essential healthcare coverage for which you or your loved one may qualify.
Listed Questions and Answers
What is the purpose of the Care 1st Arizona Prior Authorization form?
The Care 1st Arizona Prior Authorization form is designed to gather essential information for individuals with disabilities who are employed, at least 16 but not yet 65 years old, seeking healthcare coverage. This comprehensive document facilitates the evaluation of eligibility for Medicaid under specific conditions, promoting an equitable access to necessary medical services for those in need.
What information do I need to provide when filling out the form?
When completing the form, you must offer a detailed account of personal and spousal information (if applicable), without the obligation to disclose your spouse's Social Security Number if they are not applying. Additionally, employment details, including gross income and proof thereof, are required. Information about other sources of income, existing health insurance, assets, and resources must also be succinctly presented. Mention of any Social Security Disability or Supplemental Security Income benefits, details about your disability, and contact information for medical providers are also essential. Accurate, truthful responses ensure the integrity of the application process and subsequent evaluations.
Is it necessary to provide information about race or ethnicity on the form?
Disclosing race or ethnicity information on the form is entirely voluntary. The provided options aim to capture a diverse demographic landscape, yet opting out from this section will not adversely affect the application process. The selection or omission of this data is a personal choice and should align with the applicant's comfort and privacy preferences.
What happens if I fail to provide complete information or knowingly provide false information?
Submitting an application that is incomplete or contains false information may lead to receiving health benefits for which you are not eligible, potentially resulting in legal repercussions for fraud. Such actions necessitate the repayment of any erroneously paid medical bills and can jeopardize future eligibility for Medicaid benefits. Accuracy, honesty, and transparency are paramount throughout the application process to avoid these serious consequences.
How can I seek assistance if I have difficulties filling out the form or require an interpreter?
If challenges arise during the completion of the form, or if an interpreter is needed due to language barriers, support is readily available. Applicants are encouraged to contact their local Medicaid office or the provided toll-free number for assistance. Additionally, for individuals who are deaf or have hearing problems, a dedicated TTY line is accessible, ensuring comprehensive support and facilitating a smoother application process for everyone.
Common mistakes
When applying for healthcare coverage through Care 1st Arizona, specifically for persons with disabilities who are working and between the ages of 16 and 64, applicants are required to fill out a detailed prior authorization form. Although this document is crucial in determining the applicant's eligibility and need for services, several common mistakes can jeopardize the process. Identifying and avoiding these errors can significantly enhance the likelihood of approval and expedite the overall process.
-
Not Providing Complete Information:
One major error is leaving sections of the form blank. Applicants are instructed to fill out every item, indicating "none" or "0" where applicable. If a question does not apply or the answer is zero, explicitly stating so is better than leaving the space empty. This clarity helps prevent misunderstandings about whether the applicant overlooked a question.
-
Failure to Submit Required Documentation:
Another common mistake involves not including necessary proof and documents alongside the application. For income verification, for example, applicants must send copies of paycheck stubs, tax forms for self-employment, or other relevant financial documents. Neglecting to provide these can delay the process or lead to a denial due to incomplete information.
-
Incorrect Language Selection:
-
At the very beginning of the form, applicants are asked about their preferred language for communication. Failing to specify a language or incorrectly assuming services will automatically be provided in English can lead to important information being misunderstood or missed entirely if the applicant is not fully proficient in English.
-
-
Oversights in Reporting Assets and Income:
Underreporting or failing to accurately disclose assets and income is a serious mistake. The form requires detailed information about not only the applicant’s employment and salary but also about any additional sources of income and assets. This includes checking and savings accounts, retirement accounts, property other than one's home, and more. Transparency in these sections is crucial for an accurate assessment of eligibility.
Ensuring accuracy, completeness, and transparency when filling out the Care 1st Arizona Prior Authorization form is imperative. The goal is to provide the reviewing agency with a clear and full picture of the applicant's financial, employment, and health status. Avoiding these common mistakes can aid in a smoother application process, leading to faster and more favorable outcomes.
Documents used along the form
When completing the Care 1st Arizona Prior Authorization form, it's common to encounter several other forms and documents essential for a comprehensive understanding or fulfillment of requirements. These additional documents not only facilitate the authorization process but also ensure any associated actions are comprehensively addressed.
- Proof of Income Documentation: This includes pay stubs, tax returns, or official letters, providing evidence of income as stated in the application. It helps in verifying financial eligibility for Medicaid.
- Proof of Citizenship or Legal Residence: Documents such as a birth certificate, passport, or green card confirm the applicant's legal status in the United States. This is crucial for determining eligibility for the Medicaid Purchase Plan.
- Medical Documentation: Letters or reports from healthcare providers detailing the applicant's disability status and need for specific healthcare services. This documentation supports the request for Prior Authorization for specific treatments or services.
- Medicare or Other Health Insurance Cards: Proof of existing coverage is necessary to identify any primary insurance that needs to be billed before Medicaid.
- Proof of Assets: Statements or official records showcasing checking/savings account balances, property values, and other assets verify financial status and eligibility.
- Employment Verification Letter: This letter from an employer confirms the applicant's employment status and income details, providing a comprehensive view of financial resources.
- Prescription Documentation: For medications requiring prior authorization, detailed prescriptions from healthcare providers specify the need for particular drugs or dosages.
- Proof of Residence: Utility bills or a lease agreement confirm the applicant's address, an essential step to ensure they are applying in the correct state or region.
- Authorization for Release of Information: This form allows Medicaid to obtain necessary information from employers, banks, and medical providers to verify the details provided in the application.
- Disability Determination Forms: Used when an applicant is applying due to disability, these forms, filled out by medical professionals, detail the nature and extent of the disability.
These documents work together to paint a full picture of an applicant's situation, not just supporting the initial application but ensuring that all relevant aspects of their healthcare and financial situation are properly managed. Bearing in mind the sensitive nature of this information, it's advised to handle these documents carefully and understand their role in the broader process of obtaining health coverage and services.
Similar forms
The Care 1st Arizona Prior Authorization form bears resemblance to other healthcare and bureaucratic documents, like the Medicaid Application Form. Both forms seek detailed personal, financial, and health-related information to determine eligibility for services. These forms typically require the applicant's name, address, social security number, income details, and health coverage status, ensuring that the most accurate assistance is provided based on the recipient's current situation.
Similarly, the Health Insurance Marketplace Application mirrors the Prior Authorization form in gathering personal information, employment, and income details to establish eligibility for insurance plans. This process allows individuals and families to shop for insurance that meets their needs while potentially qualifying for government subsidies to reduce cost. Both documents play crucial roles in connecting individuals with affordable healthcare options.
The Disability Benefits Application Form from the Social Security Administration also shares common elements with the Prior Authorization form by collecting extensive personal and medical information. Applicants must detail their medical conditions and how these impact their ability to work, paralleling the requirement on the Prior Authorization form to detail the applicant’s disability and the need for specific healthcare services or medications.
The Employment Verification Form is another document that resembles the Prior Authorization form in its collection of employment details for financial verification purposes. While primarily used by employers or landlords to verify an individual's employment status and income, the focus on accurate and up-to-date employment data reflects the Prior Authorization form’s requirement for similar information to assess eligibility for health services or coverage.
Income Tax Return forms, like the IRS Form 1040, also share similarities with the Prior Authorization form by requiring detailed financial information from the applicant. Both forms assess the individual’s or family’s income levels which help in determining eligibility for programs or benefits, ensuring that aid is directed to those who qualify based on financial criteria.
The Health Insurance Claim Form, used by healthcare providers to bill insurers, indirectly relates to the Prior Authorization form. Both require detailed information about the medical services provided or prescribed, highlighting the necessity for specific treatments or medications and the need for such interventions to be covered under the patient's health plan.
Lastly, the Application for Supplemental Security Income (SSI) is similar to the Prior Authorization form. It targets individuals with disabilities or who are aged and in need of assistance, requiring thorough details on one’s medical condition, financial status, and living situation to ensure the provision of necessary financial support and healthcare services.
These documents, while serving different purposes across healthcare and financial assistance landscapes, collectively embody the intricacies of determining eligibility, ensuring accurate provision of services, and facilitating essential support to diverse populations.
Dos and Don'ts
When filling out the Care 1st Arizona Prior Authorization form, it is essential to pay close attention to the details and provide accurate information to avoid any issues with your application. Here are some do’s and don’ts to consider:
Things You Should Do:
- Ensure all information is accurate and truthful. Providing false or misleading information can lead to penalties, including denial of benefits or legal action.
- Include proof of income and any other required documents. Supporting documents are crucial for verifying the information on your application and determining your eligibility.
- Review the entire form before submission to ensure that no items have been missed. Completing every section accurately helps avoid delays in the processing of your application.
- If you speak or write in a language other than English, indicate your preferred language on the form to receive assistance and ensure effective communication.
Things You Shouldn't Do:
- Do not leave any questions unanswered. If a question does not apply to you, write “none” or “0” as the form instructs, rather than leaving it blank.
- Avoid guessing when providing financial details or other specific information. Estimates can lead to inaccuracies and potentially affect your eligibility or the amount of benefits you receive.
- Do not forget to sign the form. An unsigned application may not be processed, leading to unnecessary delays in receiving benefits.
- Refrain from sending original documents unless specifically required. It's often preferable to send copies of important documents to prevent loss or damage.
Misconceptions
When it comes to navigating the intricacies of healthcare coverage, particularly with forms like the Care 1St Arizona Prior Authorization form, confusion often arises. Misunderstandings can lead to delays in care, unnecessary stress, and potential financial implications. To clarify, here are ten common misconceptions:
- Only English speakers can complete the form: The form inquires about the applicant's preferred language for speaking and writing, offering assistance in languages besides English, including Spanish and Vietnamese. Interpreter services are available at no cost.
- Disability is a disqualifier: Contrary to being a disqualifier, this application specifically caters to individuals with disabilities who are employed, between the ages of 16 and 65, seeking healthcare coverage.
- Spousal information is mandatory: While the form asks about a spouse, providing a spouse's Social Security number is not required if they are not applying. The information is used only for asset verification purposes.
- Race information must be disclosed: Disclosing race is entirely optional and is solely for demographic purposes. Applicants have the liberty to omit this information without affecting their application.
- Only employed individuals are eligible: Although employment details are requested, the form also inquires about other sources of income, acknowledging various financial situations and not solely dependent on employment.
- Proof of Social Security or Unemployment income must be submitted: The form specifies that proof for these specific income types is not necessary, simplifying the process for applicants receiving such benefits.
- All assets must be disclosed: Only relevant assets or resources are required to be disclosed. This information helps in assessing eligibility without necessitating an exhaustive list of personal belongings.
- Having Medicare or other health insurance disqualifies applicants: The presence of other health insurance options, including Medicare, does not disqualify an applicant. Instead, details about such coverage are requested for a comprehensive understanding of the applicant's insurance landscape.
- Applicants with existing health conditions are ineligible: The form explicitly asks for information about disabilities and medical providers, indicating that individuals with existing health conditions are indeed encouraged to apply.
- The application is only for Medicaid: While it is an application to receive healthcare coverage, it mentions the possibility of applying for other Medicaid coverage, signifying its role as part of a broader healthcare application process.
Clarifying these misconceptions is crucial in ensuring that individuals seeking healthcare coverage through the Care 1St Arizona Prior Authorization form are adequately informed and can navigate the process with confidence. Applicants are encouraged to understand the details and requirements of the application, seek assistance when needed, and feel reassured that there are accommodations in place to help overcome language, disability, or other potential barriers.
Key takeaways
Filling out the Care 1st Arizona Prior Authorization form accurately is crucial to ensure timely and effective healthcare coverage for those who qualify. Below are key takeaways to guide you through the process:
- Ensure the form is completed in its entirety. A fully filled form prevents delays. If a question does not apply, mark it as "none" to indicate you have not skipped it accidentally.
- Interpreter services are available at no cost for non-English speakers, highlighting the importance of access to necessary resources in one’s preferred language for completing the form.
- For individuals with disabilities who work, this form is a step towards securing healthcare coverage, making accurate completion critically important for eligibility.
- When it comes to personal information such as Social Security numbers for spouses and race, provision is voluntary. This information, if provided, aids in the verification process but is not mandatory for form completion.
- Documentation of income is required. This includes paycheck stubs or tax forms for the self-employed. Accurate income reporting ensures correct eligibility determination.
- If you have other health insurance, or if you're eligible for health insurance through your employer, proof of coverage and costs incurred is necessary. This helps to coordinate benefits effectively.
- The form asks detailed questions about assets and resources. Providing truthful and accurate details here, with proof of ownership and value, is crucial for an accurate assessment of Medicaid eligibility.
- Claiming a disability requires information about medical providers, emphasizing the importance of medical evidence in supporting your application.
- Understanding your rights and responsibilities as an applicant safeguards you against misunderstandings and ensures you’re aware of the need to report changes in circumstances.
- Signing the form attests to the truthfulness of the information provided and your understanding that falsely reporting information or failing to report changes can have serious consequences, including potential legal action.
By keeping these key points in mind, applicants can navigate the process with a better understanding of what is expected, which in turn can help expedite the eligibility determination for healthcare coverage.
More PDF Forms
Undesignated Felony - An essential aspect of the application process is the notification of the prosecuting agency, ensuring all relevant parties are informed and can participate in the legal proceedings.
Arizona Income Tax Forms - The form requires identification of owners, partners, corporate officers, or officials, including their social security numbers, as part of the application process.